
Translate this page into:
Aligning vision: A case of strabismus correction combined with cataract surgery with toric extended depth of focus intraocular lens implantation

*Corresponding author: Dr. Parikshit Gogate, Department of Ophthalmology, D. Y. Patil Medical College, Pune, Maharashtra, India. parikshitgogate@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kamdar GA, Agrawal T, Gogate PM, Radhakrishnan OK. Aligning vision: A case of strabismus correction combined with cataract surgery with toric extended depth of focus intraocular lens implantation. Glob J Cataract Surg Res Ophthalmol. doi: 10.25259/GJCSRO_52_2024
Abstract
In clinical practice, it is relatively common to encounter patients with strabismus, astigmatism and cataracts. Clinicians often face the challenge of determining whether to address these conditions in separate surgical sessions or to combine them into a single procedure. This case report shares our experience regarding the clinical profile of the patient, the surgical technique employed and the postoperative outcomes related to strabismus, cataract and astigmatism were optimised to ensure the best-unaided vision for both distance and near, along with achieving perfect ocular alignment.
Keywords
Cataract surgery
Combined surgery
Esotropia
Extended depth of focus toric intraocular lens
Stereopsis
Strabismus surgery
Surgical success rate
Toric intraocular lens
Unaided vision
Visual acuity

INTRODUCTION
The simultaneous treatment of cataracts and strabismus presents significant advantages in ophthalmic care, allowing for an integrated approach that improves both visual clarity and ocular alignment in a single surgical intervention.[1-4] Conventionally, patients have undergone separate procedures for each condition, leading to extended recovery times and multiple anaesthetic exposures. The existing literature reports strabismus surgery combined with cataract surgery with monofocal intraocular lens (IOL).[1-5] By incorporating toric extended depth of focus (EDOF) IOL implantation with strabismus surgery, we can effectively manage astigmatism and cataracts to ensure the best unaided near and distance vision while simultaneously correcting eye misalignment.
This combined strategy not only lessens the overall burden on patients but also enhances their quality of life by accelerating visual rehabilitation. This case reports our experience with implanting a toric trifocal IOL following cataract surgery combined with the management of esotropia using a recess-resect procedure.
CASE REPORT
A healthy male physician in his late 60s presented to the ophthalmology outpatient clinic with complaints of inward deviation of the right eye for the past decade, alongside a gradual, painless decline in vision over the past 20 years. He reported no episodes of double vision and mentioned a history of spectacle use 50 years ago, after which he underwent bilateral photo-refractive keratectomy at the age of 35 years. In addition, he had a 20-year history of diabetes mellitus and hypertension, for which he was receiving treatment.
Upon examination, his best-corrected visual acuity (BCVA) in the right eye was 20/40 partial with a prescription of +2.50 D and −1.25 cylinder at an 80° axis for distance vision, while the left eye achieved 20/20. Near and colour vision, assessed using the Ishihara chart, were normal. Extraocular movements were full and painless, with intraocular pressures within normal limits. The Hirschberg corneal reflex test indicated 30° of esotropia, and the cover-uncover test revealed alternating esotropia with left eye dominance [Figure 1]. The prism bar cover test demonstrated 60 prism dioptres of esotropia in the right eye across all gazes. Stereoacuity testing yielded 160 s of arc, and Schirmer testing was also within normal limits. The IOL power was calculated with the Barrett True-K IOL formula after ascertaining keratometry, anterior chamber depth and axial length using an optical biometer (IOL master 700 by Zeiss Inc.).
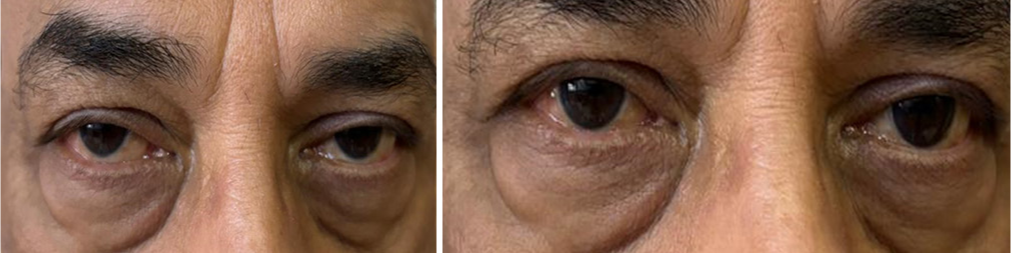
- Showing pre operative image.
The patient underwent right eye medial rectus recession of 5 mm and lateral rectus resection of 6 mm, along with toric EDOF IOL (Technis Eyhance toric, Jhonson and Jhonson), all performed under local anaesthesia by one of the authors (PG). The strabismus surgery was done first, followed by cataract surgery. Four cardinal meridians were marked pre-operatively. The IOL alignment was to be at 124° with the temporal incisio n. A small nick on the limbus marked this before starting the strabismus surgery. The cataract procedure commenced 25 min after the strabismus procedure and the cornea was slightly hazy due to exposure [Figures 2 and 3]. In hindsight, we should have covered the cornea not just with a moist cotton swab but rather with moist gauze and viscoelastic during the strabismus surgery.
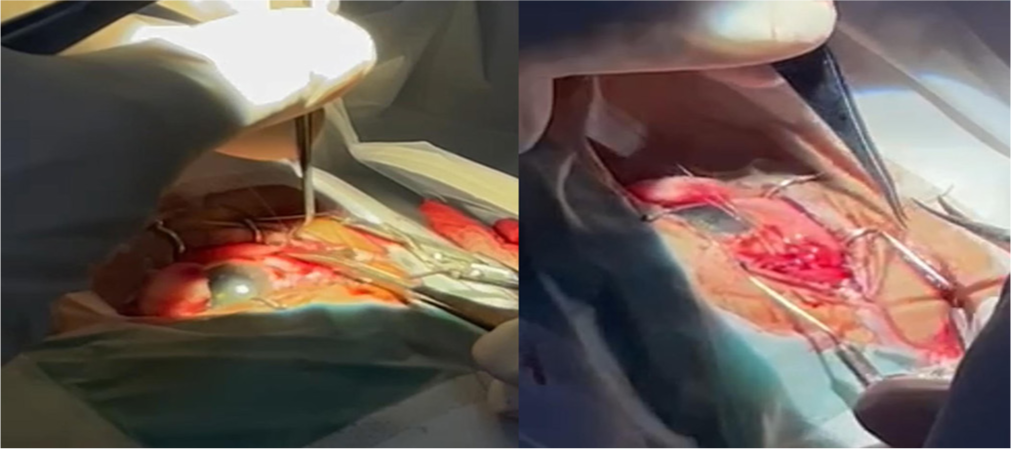
- Showing intra operative image of squint surgery.

- Showing Intraocular implantation of lens.
On the 1st postoperative day, the BCVA in the operated eye improved to 20/40 with a cylinder of −1.0° at a 120° axis. Residual esotropia was measured at 8 prism dioptres, and intraocular pressure was recorded at 20 mmHg in the right eye. The patient’s IOL was at 110° and was subsequently redialled to 124° on the second post-operative day, resulting in BCVA improvement to unaided 20/20 for distance and N6p for near with orthophoria within 2 days.
Postoperatively, the patient was prescribed prednisolone eye suspension 1% every 3 h, moxifloxacin 0.5% 4 times a day, nepafenac 0.1% 3 times a day and carboxymethylcellulose 0.5% 4 times a day. At the 7-week follow-up, the patient maintained unaided 6/6p for distance and N6 for near vision with 2 prism diopter (2PD) esotropia for near and orthophoria for distance [Figure 4].
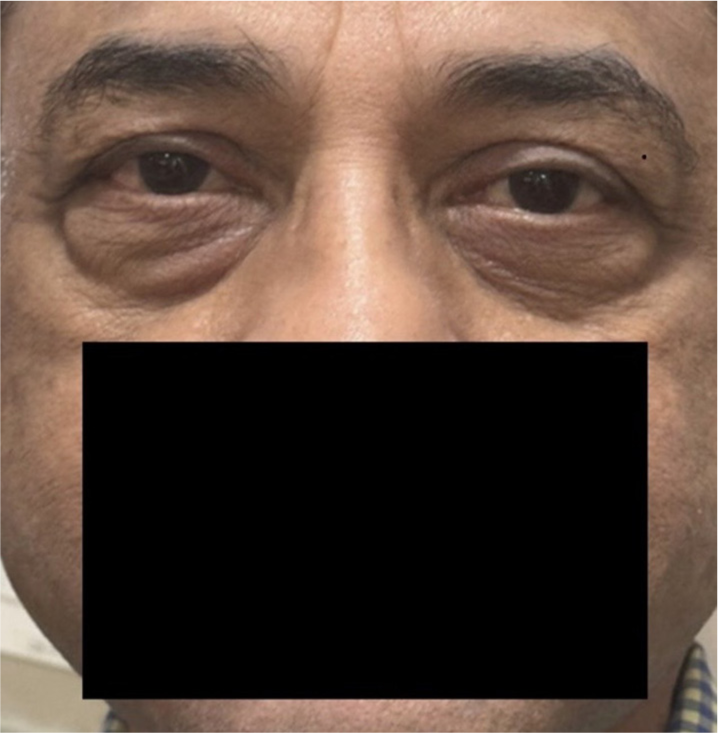
- Showing post operative image.
DISCUSSION
Cataracts and strabismus are commonly encountered conditions in ophthalmology. While the benefits of combined surgeries for vitreoretinal and cataract issues, as well as glaucoma and cataract, are well established, there are few reports on the simultaneous performance of cataract and strabismus surgeries.[1-6] The first documented case of combined cataract and strabismus surgery was reported by Maltzman et al.,[1] who studied 10 patients suffering from significant concomitant exotropia and cataracts. Their findings indicated that this dual approach was safe and facilitated quicker visual rehabilitation for patients compared to performing the surgeries separately.[1]
Another report focused primarily on a paediatric population, detailing various combined procedures. Of the 10 cases examined, 9 involved patients younger than 14 years, most of whom had poor visual prognoses due to congenital issues or trauma.[1] Only one adult patient in this study had a reasonable chance for visual improvement; however, details on this case were limited, and the impact of strabismus surgery on alignment was not clarified.
In our practice, we performed combined strabismus surgery and phacoemulsification cataract surgery with toric EDOF IOL implantation. Postoperatively, we observed significant improvement in visual acuity in the treated eye, resulting in an aligned visual axis that resolved symptomatic diplopia. There was an improvement in the cosmetic appearance of the strabismus.
Indications for combined surgery in patients with cataracts and strabismus include: (1) enhancing visual acuity, motor fusion and binocular single vision in individuals experiencing symptomatic cataracts and diplopia; (2) aligning a mechanically misaligned eye with good visual potential to enable small-incision cataract surgery and (3) minimising the number of surgeries required for high-risk or elderly patients.[2] For selected individuals with symptomatic cataracts and strabismus, combined surgery is a viable option. Advances in small-incision cataract techniques and modern strabismus procedures now allow these surgeries to be performed safely and effectively together. We were apprehensive that the post-operative astigmatism would not be entirely predictable and reduce the efficacy of the toric EDOF implant. However, this proved to be unfounded. Basmak et al. had done the strabismus surgery with adjustable sutures to obviate this problem.[6] If the visual acuity due to cataract would have been very poor, <3/60 then it would be difficult to assess whether strabismus was co-existing or had developed due to poor vision (sensory strabismus) and strabismus measurement with prism bar alternate cover test may not be that accurate. In such cases, a graded or two-step surgery, cataract surgery followed by strabismus surgery, if needed, would have been a better approach.
CONCLUSION
The combined strategy of cataract surgery with toric IOL implantation and strabismus correction in a single surgical session offers a valuable solution for patients with both conditions. This approach streamlines the surgical process, reducing the need for multiple interventions, while enhancing patient comfort and satisfaction through minimised recovery times. Our findings suggest that this dual procedure can effectively improve visual acuity and ocular alignment, leading to favourable postoperative results. By concurrently addressing cataracts and strabismus, we can optimise patient care, facilitate quicker visual rehabilitation and ultimately enhance the overall quality of life for our patients. Ongoing research and refinement of surgical techniques will further establish this integrated approach as a standard practice in ophthalmology.
Ethical approval
Institutional Review Board has waived the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Combined intraocular lens and strabismus surgery. J Cataract Refract Surg. 1986;12:65-8.
- [CrossRef] [PubMed] [Google Scholar]
- Combined strabismus and phacoemulsification cataract surgery: A useful option in selected patients. Eye. 2001;15:736-8.
- [CrossRef] [PubMed] [Google Scholar]
- Combined intraocular and strabismus surgery. Ophthalmic Surg Lasers. 1998;29:456-61.
- [CrossRef] [PubMed] [Google Scholar]
- Performing combined strabismus and cataract surgery: An effective approach in selected cases. Strabismus. 2008;16:5-9.
- [CrossRef] [PubMed] [Google Scholar]
- Combined cataract and strabismus surgery with adjustable sutures. Ophthalmic Surg Lasers Imaging. 2006;37:198-203.
- [CrossRef] [PubMed] [Google Scholar]




